Introduction
Musculoskeletal disorders, including knee osteoarthritis, have become one of the most relevant etiologies of disability and chronic pain. In fact, almost 40% of patients over 65 years report joint pain (1).
Despite the growing number of patients with this condition, there are still major difficulties in providing an accurate diagnosis of common musculoskeletal disorders associated with chronic pain (2).
Knee osteoarthritis (KOA) is the most common type of arthritis, and its prevalence is continuously increasing due to higher proportion of elderly patients and obesity around the world. Estimates report that up to 13% of women and 10% of men over 60 years have symptomatic KOA (3).
Current guidelines on treatment of KOA recommend a non-pharmacological approach as a first line (4). Physical therapy has demonstrated a trend in reducing pain, improving range of motion and function. Physical agents or interventions other than exercise are not recommended (5) and manual therapy has mixed recommendations in current guidelines with some not recommending it (5,6), but recent systematic reviews have shown a reduction in short term pain and an increase in range of motion and function (7,8).
In cases where there are no clinical responses with non-pharmacological approaches, pharmacological approaches with NSAIDs or intra-articular corticosteroids are the only ones with a strong recommendation but only for short term relief given the known safety issues with both treatments (4,9).
This situation leaves patients with a lack of recommended alternatives between non-pharmacological approaches and surgery, and it is within this gap that regenerative medicine aims to provide solutions.
Regenerative medicine is the field of medicine that uses the body’s healing capacity to improve recovery of tissues, treat pain and improve function by means of injection of cellular or non-cellular solutions which mobilize inflammatory cells and growth factors to restore tissue (10). Recent advances and evidence on the application of regenerative medicine for the treatment of pain from a myriad of musculoskeletal disorders have led to the publication of the first guidelines on the matter in 2024 (11) giving physicians the opportunity of knowing current state of evidence on its effectiveness and safety.
Dextrose Prolotherapy (DPT) is a type of non-cellular regenerative treatment first described by George Hackett in the mid-fifties which uses a hypertonic dextrose-based solution to stimulate inflammation and regeneration to tissues (12).
As a chapter of the International Association for the Study of Pain (IASP), the Argentine Association for the Study of Pain (AAED) is dedicated to promulgating scientific advancements in pain diagnosis and management. To this end, the AAED Special Interest Group on Musculoskeletal Pain has undertaken a narrative review to evaluate current evidence regarding the rationale, efficacy, and safety of DPT for chronic pain secondary to KOA.
Materials and methods
The intention of this review is to serve as a preliminary study for physicians not familiarized with DPT. A narrative review design was chosen for this study to cover various aspects of DPT treatment, from its mechanism of action to its clinical effectiveness. The main weakness of the design selected is its inability to conduct a meta-analysis and a proper risk of bias assessment.
We conducted a search in MEDLINE, SciELO, and Google Scholar using the following terms: (“Prolotherapy”) AND (“Osteoarthritis, Knee”).
The inclusion criteria were studies that selected adults over 18 years with KOA that were included in DPT as treatment in the setting of randomized clinical trials, non-randomized clinical trials, systematic reviews, or observational studies.
We conducted a second search on MEDLINE, Scielo and Google Scholar using the following terms:((“Prolotherapy”) AND (“Osteoarthritis, Knee)) AND “mechanism” OR “Rationale” to include articles that address the mechanism of action of DPT in KOA.
Both searches were conducted in English and Spanish between January 2005 and October 2025.
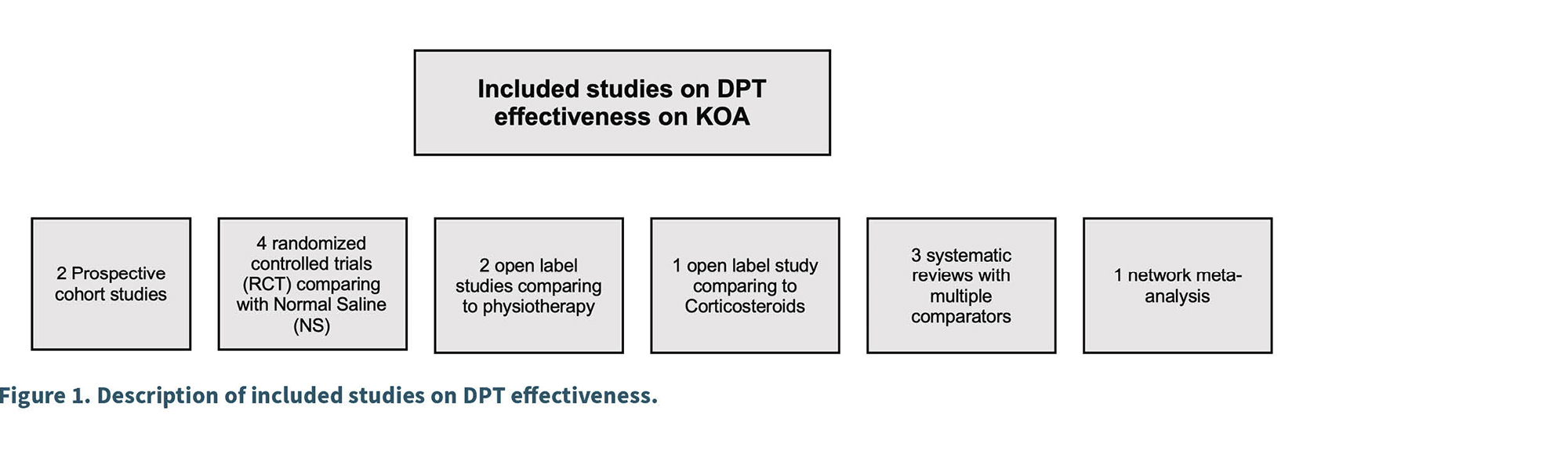
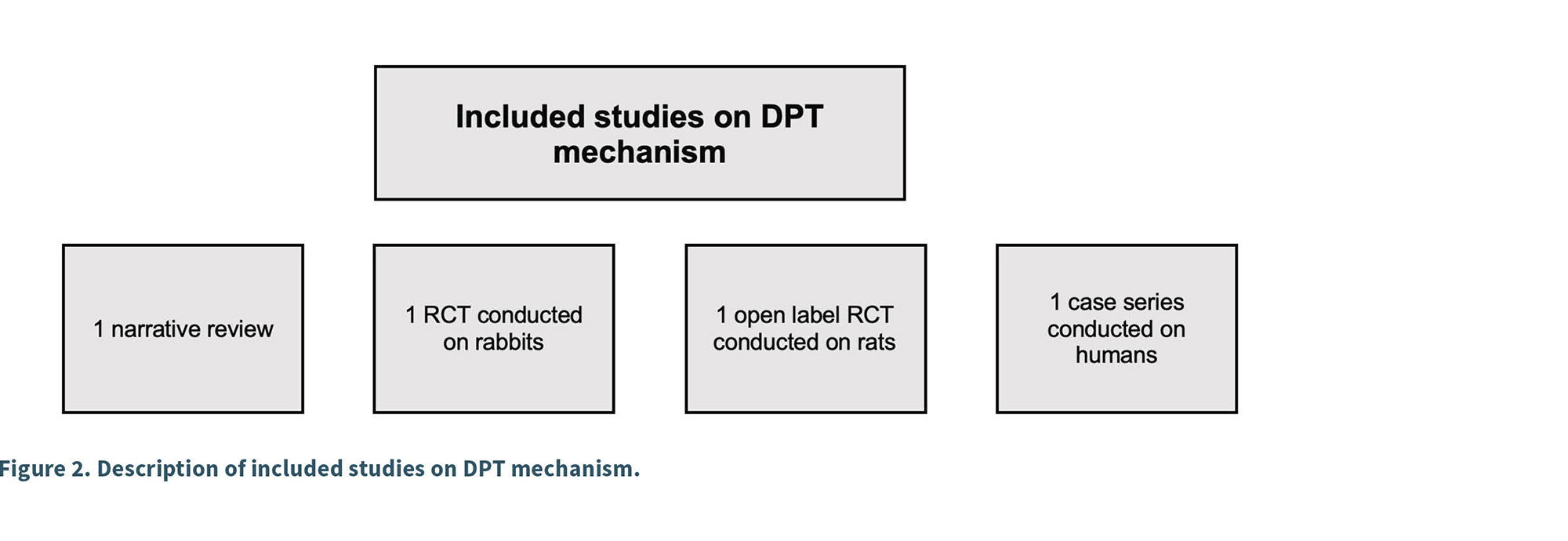
In Figures 1 and 2, we present the results from the search and the description of studies that were included in this narrative review.
Rationale and mechanism of action of prolotherapy
As previously described, DPT uses hypertonic dextrose solutions injected directly in the lesion to promote healing and alleviate pain.
The exact mechanism of action of DPT is not fully understood, but it is increasingly being investigated, as discussed in this section. Another important consideration is that DPT has been reported in the literature using different concentrations of hypertonic dextrose within a range that comes from 10% to 25% (13,14) so the appropriate dosage or concentration solution to maximize its effectiveness is uncertain.
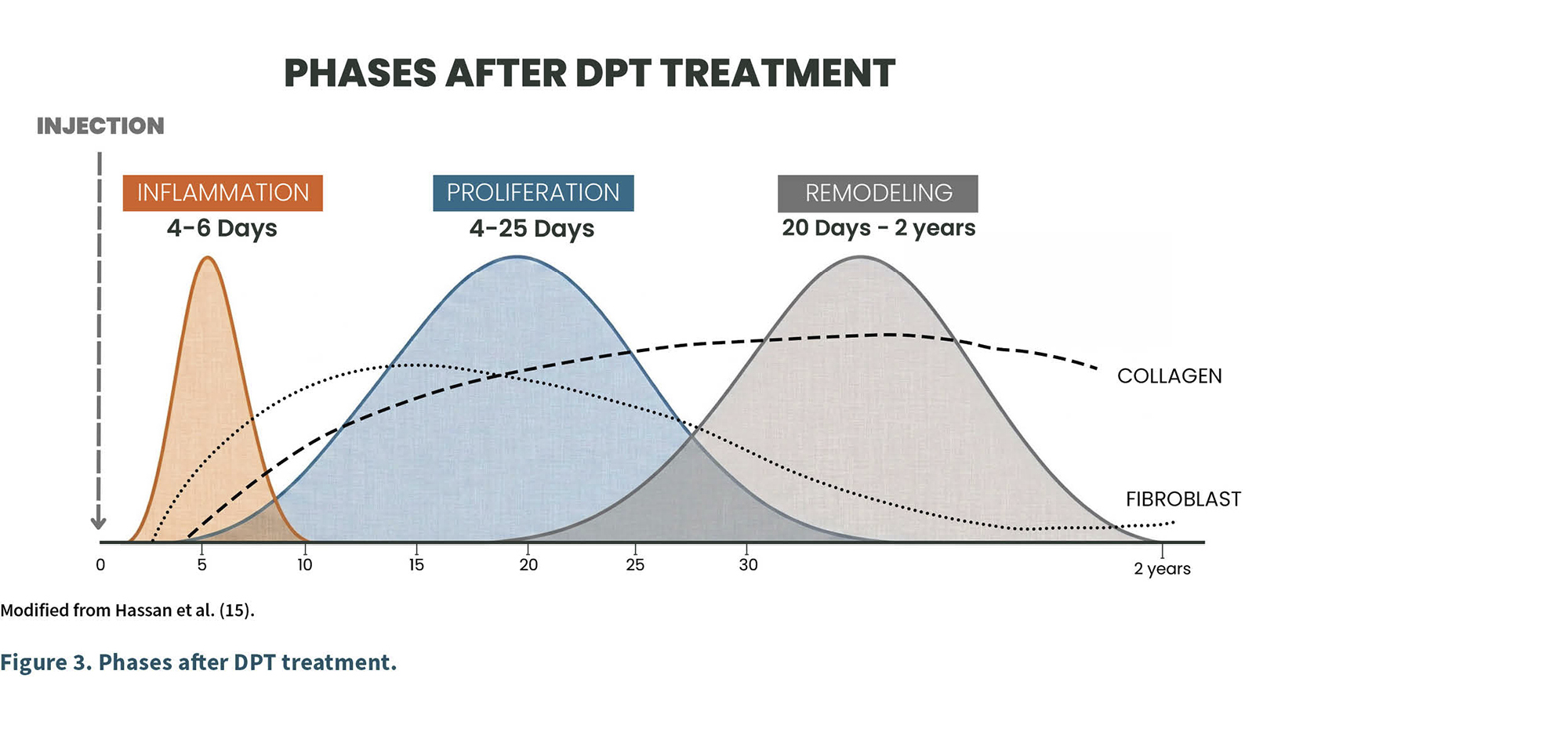
The proposed mechanism of DPT involves inflammation secondary to the effect of the hypertonic glucose effect on tissues injected by granulocytes and macrophages activation. This “controlled inflammation” leads to activation of healing of injured tissues by means of inflammatory cytokines and growth factors released within the injected area and lateral activation of fibroblasts that produce new collagen (15).
There are three distinct phases after DPT solution injection. The inflammation phase that lasts up to six days, the proliferation phase that is characterized by matrix and cellular proliferation which lasts up to twenty five days and finally the remodeling phase afterwards (16) (Figure 3).
The first study that evaluated the ability of glucose to reduce cartilage degeneration was conducted by Yoo-Sin Park et al. (17), in this study it was shown that the intra-articular injection of glucose on rabbit’s knees with anterior cruciate ligament transected exhibited lesser erosion of cartilage and a higher production of matrix on haematoxylin and eosin staining and scanning electron microscopy compared to knee joints that were injected only with NS.
Aqsa Zahid et al. (18) also evaluated histomorphology of tibial articular cartilage after intra-articular DPT on monosodium iodoacetate (MIA) induced KOA on a rat model. The rats that were exposed to 25% hypertonic dextrose presented improvement in the number of chondrocytes, thickness of articular cartilage and gross appearance.
Topol et al. (19) made novel research to further understand the mechanism underlying DPT on human subjects, they conducted a trial involving 6 patients with KOA that were given 4 cycles of 12.5% DPT with prior and after treatment arthroscopy with biopsy. All six patients had chondrogenesis on arthroscopy as measured by three arthroscopists blinded and on biopsies. We can conclude that there is a trend in the available data supporting the potential of DPT to promote cartilage growth in both animals and humans, but the exact mechanism is yet to be elucidated.
However, two specific situations should be highlighted. The first is that studies aimed at determining its mechanism of action remain scarce, and the second is that biological plausibility does not necessarily determine clinical effectiveness.
Efficacy of DPT on knee osteoarthritis treatment
In the following section, we will present the current evidence on efficacy of DPT on the management of KOA.
DPT for knee osteoarthritis; long term and functional outcomes:
Rabago et al. (20) evaluated the long-term effects of DPT for KOA in 65 adults that were previously included in three prior studies with an open-label follow-up trial assessing self-reported outcomes for up to 3.5 years after enrollment. Participants received 3–5 monthly DPT sessions and were assessed up to 2.5 years later using the WOMAC index and Knee Pain Scale (KPS). Results showed progressive improvement in pain, stiffness, and function in 62% of participants, with a mean 36% increase in WOMAC scores. KPS also improved with 86% of participants reporting less pain. No major adverse events were reported.
Waluyo et al. (21) conducted a severity-based pilot study to evaluate the effect of DPT on functional outcomes in KOA. Twenty-one participants with KL grade 1-4 OA received three sessions of intra-articular (25%) and periarticular (15%) dextrose injections at four-week intervals. Functional status was assessed with WOMAC scores at baseline and at 12 weeks. Results showed significant improvement in overall WOMAC scores (48% reduction, p < 0.001), as well as in pain and physical function subscales in both mild (KL 1-2) and moderate-severe (KL 3-4) groups. Stiffness scores showed no significant improvement in either group. No major adverse events were reported.
In accordance with both trials, DPT was shown to be a safe, well-tolerated, and effective intervention for improving function and decreasing pain but the lack of well-designed randomized clinical trials on the subject gives uncertainty on the quality of evidence and strength of this recommendation.
Randomized controlled trials
Dextrose Prolotherapy versus saline injections and exercise
Sit et al. (22) conducted a single-center, triple-blinded randomized controlled trial comparing intra-articular DPT with normal saline (NS) injections for KOA. Seventy-six participants with moderate-to-severe KOA received four ultrasound-guided injections at weeks 0, 4, 8, and 16, and were followed for 52 weeks. The primary outcome was the WOMAC pain score, with secondary outcomes including WOMAC function, stiffness, composite scores, VAS pain, quality of life (EuroQol-5D), and physical performance tests. Results showed significantly greater pain reduction in the DPT group versus NS at 52 weeks (difference-in-difference -10.3, p = 0.022), along with improvements in WOMAC function and composite scores, VAS pain and EuroQol-5D scores. Objective physical function tests improved in both groups but did not differ significantly. No procedure-related adverse events occurred, adherence was high, and 94% of DPT participants reported willingness to recommend treatment.
Sert et al. (23) conducted a three-arm randomized controlled trial to evaluate the effects of DPT compared with NS and a home-based exercise program in patients with KL grade II–III KOA. Sixty-six patients were randomized into a DPT group (PG), saline group (SG), or control group (CG). PG and SG received three intra- and periarticular injections at weeks 0, 3, and 6, while all groups performed a standardized exercise program. Primary outcome was WOMAC pain, with secondary measures including WOMAC function, stiffness, VAS pain/stiffness, and SF-36 quality of life scores, assessed at baseline, 6 weeks, and 18 weeks. Results showed significant improvements in WOMAC pain, function, stiffness, and SF-36 physical scores in PG compared to CG at 18 weeks, with greater improvements in WOMAC pain and function compared to SG. Both PG and SG showed significant short-term improvements versus CG, suggesting an active effect of injection, but PG achieved larger and clinically meaningful changes, particularly in pain reduction (6.2 points on a 0-10 VAS). No major adverse events were reported.
Rabago et al. (24) conducted a three-arm, blinded randomized controlled trial comparing DPT, NS injections, and home exercise for KOA. Ninety adults with moderate pain and radiographically confirmed KOA received injections at weeks 1, 5, and 9, with optional sessions at weeks 13 and 17, or were assigned to a standardized exercise program. Primary outcome was the WOMAC composite score, with secondary measures including the Knee Pain Scale (KPS). At 52 weeks, the DPT group had significantly greater improvement in WOMAC scores (mean change 15.3 points, 24% improvement) compared to NS (7.6 points) and exercise (8.2 points), exceeding the minimal clinically important difference. Improvements were consistent across pain, stiffness, and function subscales, with near-maximal benefit achieved by 26 weeks and maintained at 1 year. KPS scores confirmed significant pain reduction in treated knees compared to controls. No major adverse events occurred, and satisfaction with DPT was high.
But not all studies compared to NS found a superiority of DPT, Teymouri et al. (25) conducted a double-blind randomized controlled trial comparing a single ultrasound-guided intra-articular injection of 50% DPT with NS for mild-to-moderate KOA. Fifty participants (mean age 63, 70% women) completed the study and were followed for 8 weeks. Both groups showed significant improvement in WOMAC pain, stiffness, and function scores, Oxford Knee Score, VAS pain, and knee extension at all follow-up points (p < 0.001). Although the DPT group consistently showed numerically greater improvement than NS, the differences between groups were not statistically significant. No major adverse events were reported; transient injection-site pain and ecchymosis resolved by week 4.
We can conclude that most studies that evaluated DPT versus NS or exercise showed superiority of DPT. In the case of Teymouri et al. in which NS injections were not inferior, it is important to remark that it was the only study that used a single session of DPT against most protocols. Even within an inferior margin of benefit, NS showed improvements in pain and WOMAC scores, the mechanism of action on how NS can decrease pain remains to be solved but the presence of a placebo-effect cannot be overruled. Regarding exercise, DPT was superior in terms of improvement of WOMAC scores in the only study found using exercise as a direct comparator.
Dextrose prolotherapy versus physiotherapy and other conservative strategies
Yildiz et al. (26) conducted a randomized prospective trial comparing DPT with conventional physiotherapy (CPT) in 60 women with KL grade II–III KOA. Participants were randomized to receive either two sessions of combined intra- and periarticular DPT (25% and 15% dextrose, respectively) at 2-week intervals or 20 CPT sessions over 4 weeks (hot packs, TENS, ultrasound). Both groups performed a home exercise program. Outcomes included VAS pain, WOMAC scores, active knee ROM, 50-m walking time, and isokinetic quadriceps/hamstring strength measured at baseline, 1 month, and 3 months. Both groups showed significant within-group improvements in all outcomes (p < 0.001), but DPT produced greater reductions in VAS pain and larger gains in quadriceps strength and walking time at both follow-ups. WOMAC improvements favored DPT but were not statistically significant. No major adverse effects were reported.
Meena et al. (27) conducted a 12-month randomized controlled trial comparing DPT with standard non-surgical management (physical therapy, NSAIDs, hyaluronic acid injections) in 80 adults with KL grade 2-4 KOA. The DPT group received intra-articular injections at weeks 0, 4, and 8 under ultrasound guidance. Both groups were assessed for pain (VAS), function (WOMAC), knee mobility, quality of life (SF-36), and adverse events at baseline, 3, 6, and 12 months. Results showed significantly greater improvement in the DPT group for pain (VAS decreased from 7.5 to 3.0 vs. 7.0 to 4.5, p < 0.05) and function (WOMAC from 60 to 30 vs. 58 to 42, p < 0.05). Quality of life and joint mobility gains were also superior with DPT, and no serious adverse events were reported apart from mild, transient injection discomfort.
Both DPT and CPT showed to be effective on pain relief and functional improvement in KOA patients but the effect of DPT was superior on pain reduction, function, and quality of life in all included studies.
Dextrose prolotherapy versus corticosteroids
Bayat et al. (28) conducted a double-blind randomized clinical trial comparing combined intra-articular and neurofascial DPT with intra-articular triamcinolone injection in 50 patients with Kellgren–Lawrence(KL) grade II–III KOA. Participants received either a single session of DPT (10 mL 16% dextrose intra-articular + periarticular 12% dextrose at 4 points) or 40 mg triamcinolone. Outcomes (VAS pain and WOMAC total, pain, stiffness, and function) were measured at baseline, 1 month, and 3 months. Both groups showed significant improvement at 1 and 3 months (p < 0.001). At 1 month, pain reduction favored corticosteroid, but by 3 months, DPT showed significantly greater improvement in pain (VAS and WOMAC), stiffness, function, and total WOMAC score (p < 0.001). No serious adverse events were reported.
This is the only trial that compared DPT with corticosteroids for the treatment of symptomatic KOA, the fact that Triamcinolone gave a better short-term relief but not in mid-term against DPT could be related to the initial inflammation phase after a DPT treatment that could give patients a higher amount of pain in comparison of triamcinolone which gives rapid decrease on pain and inflammation. The mid-term benefit of DPT over Triamcinolone is probably secondary to the start of remodeling after the inflammatory and proliferative phase of regenerative medicine and the decreasing over-time effect of triamcinolone.
Differences on Dextrose prolotherapy protocols among included studies
As previously stated, one of the main limitations of the DPT studies is the wide variety of treatment protocols used, Table I summarizes the differences in the DPT protocols used on the analyzed studies.
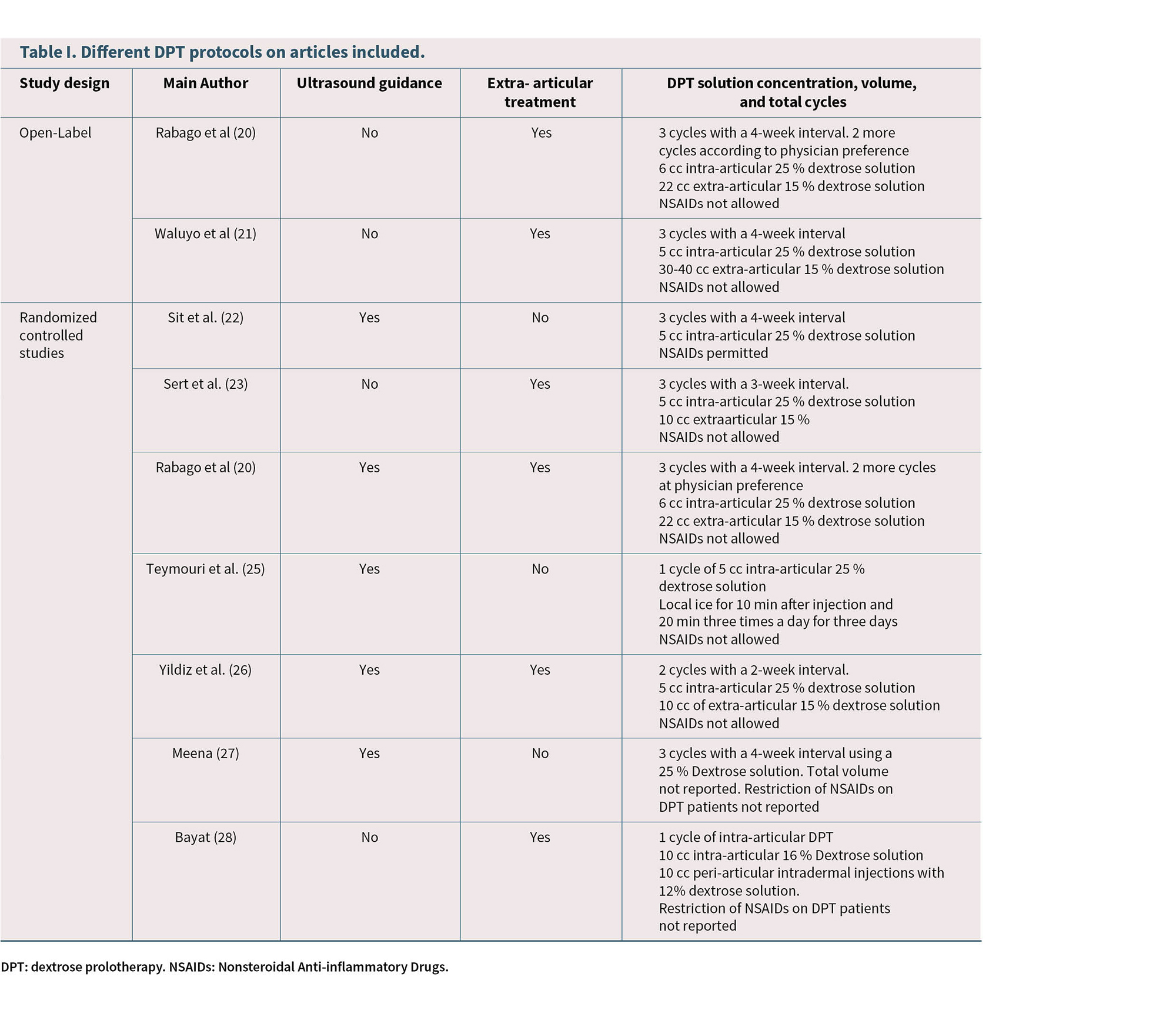
We found differences on the number of cycles, the concentration of dextrose used, the total volumes injected, ultrasound guidance use and the restriction on NSAIDs use among included studies.
Systematic reviews evaluating DPT compared with other interventions for KOA
Several systematic reviews have been made regarding effectiveness of DPT on symptomatic KOA, in this section we will summarize the most relevant ones.
Arias-Vázquez et al. (29) conducted a systematic review of ten randomized controlled trials (n = 676) comparing hypertonic DPT with other intra- or periarticular interventions for KOA. Across studies, DPT was more effective than local anesthetic placebo injections for pain and function improvement, showed comparable efficacy to hyaluronic acid, ozone therapy, and radiofrequency, but was slightly less effective than platelet-rich plasma (PRP) and erythropoietin at 6-month follow-up. The benefits of DPT were observed in the short, medium, and long term, with some studies reporting sustained improvement up to 12 months and even 2.5 years. Adverse effects were minimal, limited to mild transient pain or swelling, with no serious complications reported.
Wee et al. (30) performed a systematic review and meta-analysis of 11 randomized controlled trials (n = 837) evaluating DPT for KOA. Most studies used intra-articular dextrose injections (10-25%), often in a three-session protocol, with follow-up ranging from 3 to 12 months. Meta-analysis showed that DPT improved pain and function compared to placebo and some active controls, though results were heterogeneous, and many trials had a high risk of bias. When compared with platelet-rich plasma (PRP), DPT showed similar short-term effects on pain and function but was slightly inferior for stiffness at six months. Compared to hyaluronic acid, both treatments improved pain and WOMAC scores, with HA showing greater benefit in one study. Adverse events were minimal and self-limited (transient pain, bruising).
Waluyo et al. (31) conducted a systematic review of clinical trials assessing DPT for KOA. The included studies consistently demonstrated significant pain reduction and functional improvement, often surpassing placebo and local anesthetic controls. Some trials found results comparable to hyaluronic acid injections and physiotherapy, while others reported slightly inferior outcomes compared to platelet-rich plasma (PRP). Treatment protocols generally involved 3-5 sessions of intra- and periarticular injections with dextrose concentrations between 10-25%, spaced over several weeks. Reported adverse effects were mild, transient, and self-limited, such as post-injection pain and swelling.
Network meta-analysis of combined treatments
Liao et al. (32) conducted a network meta-analysis of 80 randomized controlled trials (n = 6,934) comparing intra-articular injections (IAI), physical therapy (PT), and their combination (IAI + PT) in KOA. Interventions included corticosteroids, hyaluronic acid, platelet-rich plasma, mesenchymal stem cells, ozone, and DPT, either alone or combined with PT (exercise, physical agents, or activity training). Results showed that combined regimens outperformed monotherapies for pain, global function, and walking capability. DTP + PT ranked highest for pain reduction (SUCRA 0.93) and global function restoration (SUCRA 0.85), while MSC+PT was most effective for walking capability (SUCRA 0.84). Subgroup analyses indicated that combined therapies-maintained superiority across immediate, short-, medium-, and long-term follow-up. No serious adverse events were reported, and compliance was high.
Discussion
Regenerative medicine is growing in the field of musculoskeletal pain of different etiologies, in relation of the latter, DPT is advancing in the same way and is becoming more available and with a rising number of trials published in recent years on multiple pathologies beyond KOA (33-35). Several studies have shown that it seems to be less effective in treating pain than PRP (29-31), but its superiority arises in that it doesn’t need equipment for sample collecting or an experienced haemotherapist.
This advantage makes DPT an affordable option for patients and easier for physicians to implement. The choice between these two strategies ultimately boils down to a balance between the possibility of obtaining the PRP sample in a biosafety-compliant environment, the cost of both procedures, and the clinical significance the physician assigns to the change in terms of the PRP superiority shown on studies.
Systematic reviews represent the most reliable study design to strengthen recommendations for any given clinical practice, DPT has multiple systematic reviews and network meta-analysis on the treatment of KOA as was previously shown, with this information previously described we can conclude that DPT appears to be safe due to its minimally invasive nature, lack of serious adverse events reported and effectiveness on the improvement of pain and function of symptomatic KOA patients, even when compared to other strategies. Nonetheless, this evidence is limited by methodological heterogeneity of trials that gives risk of bias so there’s need for higher quality randomized controlled trials to further recommend DPT as a first line therapy.
DPT could be an effective and safe alternative for patients that are in the gap between the lack of benefit of conservative management and knee replacement surgery due to the alleged superiority over conservative and minimally invasive treatments like corticosteroids (28) or hyaluronic acid (27, 29-31).
This review shows that DPT has enough evidence nowadays to separate it from the notion that it is an “alternative medicine” procedure. Nevertheless, DPT is a complementary treatment that is not meant to be solitary but in combination with physical therapy’s evidence-based interventions.
Regardless of the latter, it is important that patients and physicians know that to this date, there is no consensus regarding a specific protocol for each pathology, so this heterogeneity of dextrose concentrations and specific targets gives uncertainty and difficulty to conduct proper randomized clinical trials to assess effectiveness. This heterogeneity is not to be solved soon because the population that is encompassed within KOA pain is in fact a population that have a myriad of etiologies of “gonalgia” including multiple insertional entesopathies, neuropathic pain and not only somatic pain arising from cartilage (36), so the protocol of every patient may differ given that DPT is a treatment that needs to be patient centered involving the evaluation of every aspect that could give knee instability to any given patient and then choose adequate treatment targets.
Finally, DPT has a potential role in the management of patients with KOA who are refractory to conservative treatment regarding its effectiveness on studies and there is biological plausibility of its mechanism on animal and human models but there are still need for more evidence to give DPT a stronger recommendation.
Conflict of interest
None to declare.
Funding
None.
references
1. Malik KM, Beckerly R, Imani F. Musculoskeletal Disorders a Universal Source of Pain and Disability Misunderstood and Mismanaged: A Critical Analysis Based on the U.S. Model of Care. Anesth Pain Med. 2018;15;8(6):e85532. DOI: 10.5812/aapm.85532.
2. Hendler N. Why Chronic Pain Patients are Misdiagnosed 40 to 80 % of the Time? J Rec Adv Pain. 2016;2(3):94-8. DOI: 10.5005/jp-journals-10046-0051.
3. Mintarjo JA, Poerwanto E, Tedyanto EH. Current Non-surgical Management of Knee Osteoarthritis. Cureus. 2023;15(6):e40966. DOI: 10.7759/cureus.40966.
4. Kolasinski SL, Neogi T, Hochberg MC, Oatis C, Guyatt G, Block J, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Rheumatol. 2020;72(2):220-33. DOI: 10.1002/art.41142.
5. Van Doormaal MCM, Meerhoff GA, Vliet Vlieland TPM, Peter WF. A clinical practice guideline for physical therapy in patients with hip or knee osteoarthritis. Musculoskeletal Care. 2020;18(4):575-95. DOI: 10.1002/msc.1492.
6. Dantas LO, Salvini TF, McAlindon TE. Knee osteoarthritis: key treatments and implications for physical therapy. Braz J Phys Ther. 2021;25(2):135-46. DOI: 10.1016/j.bjpt.2020.08.004.
7. Tsokanos A, Livieratou E, Billis E, Tsekoura M, Tatsios P, Tsepis E, et al. The Efficacy of Manual Therapy in Patients with Knee Osteoarthritis: A Systematic Review. Medicina (Kaunas). 2021;57(7):696. DOI: 10.3390/medicina57070696.
8. Feng T, Wang X, Jin Z, Qin X, Sun C, Qi B, et al. Effectiveness and safety of manual therapy for knee osteoarthritis: An overview of systematic reviews and meta-analyses. Front Public Health. 2023;11:1081238. DOI: 10.3389/fpubh.2023.1081238.
9. Magni A, Agostoni P, Bonezzi C, Massazza G, Menè P, Savarino V, et al. Management of Osteoarthritis: Expert Opinion on NSAIDs. Pain Ther. 2021;10(2):783-808. DOI: 10.1007/s40122-021-00260-1.
10. Kaye AD, Edinoff AN, Rosen YE, Boudreaux MA, Kaye AJ, Sheth M, et al. Regenerative Medicine: Pharmacological Considerations and Clinical Role in Pain Management. Curr Pain Headache Rep. 2022;26(10):751-65. DOI: 10.1007/s11916-022-01078-y.
11. D’Souza R, Her Y, Hussain N, Karri J, Schatman M, Calodney A, et al. Evidence-Based Clinical Practice Guidelines on Regenerative Medicine Treatment for Chronic Pain: A Consensus Report from a Multispecialty Working Group. J Pain Res. 2024;17:2951-3001. DOI: 10.2147/JPR.S480559.
12. Reeves KD, Sit RW, Rabago DP. Dextrose Prolotherapy. Phys Med Rehabil Clin N Am. 2016;27(4):783-823. DOI: 10.1016/j.pmr.2016.06.001.
13. Hauser RA, Lackner JB, Steilen-Matias D, Harris DK. A Systematic Review of Dextrose prolotherapy for chronic musculoskeletal pain. Clin Med Insights Arthritis Musculoskelet Disord. 2016:9:139-59. DOI: 10.4137/CMAMD.S39160.
14. Distel LM, Best TM. Prolotherapy: A Clinical Review of Its Role in Treating Chronic Musculoskeletal Pain. PM R. 2011;3(6 Suppl 1):S78-81. DOI: 10.1016/j.pmrj.2011.04.003.
15. Hassan RE, Ahmad Y, Haroon H, Khan AU, Abbasi M. Hypertonic Dextrose Prolotherapy for Knee Osteoarthritis: A Comprehensive Review of Mechanism, Techniques, Limitations, and Side Effects. J Islamabad Med Dental Coll. 2024;13(2):375-80. DOI: 10.35787/jimdc.v13i2.1245.
16. Trescot A. Everything old is new again: New developments in prolotherapy. Tech Reg Anest Pain Manag. 2015;19(1-2):14-8. DOI: 10.1053/j.trap.2016.09.003.
17. Park YS, Lim SW, Lee IH, Lee TJ, Kim JS, Han JS. Intra-articular injection of a nutritive mixture solution protects articular cartilage from osteoarthritic progression induced by anterior cruciate ligament transection in mature rabbits: a randomized controlled trial. Arthritis Res Ther. 2007;9(1):R8. DOI: 10.1186/ar2114.
18. Zahid A, Qamar K, Mehwish Abaid AT, Bashir Kiani MR, Aslam M. Ameliorative Effects of Prolotherapy on Histomorphology of Tibial Articular Cartilage of Chemically Induced Osteoarthritic Knee Joint in a Rat Model. J Coll Physicians Surg Pak. 2023;33(8):836-41. DOI: 10.29271/jcpsp.2023.08.836.
19. Topol GA, Podesta LA, Reeves KD, Giraldo MM, Johnson LL, Grasso R, et al. Chondrogenic Effect of Intra-articular Hypertonic-Dextrose (Prolotherapy) in Severe Knee Osteoarthritis. PM R. 2016;8(11):1072-82. DOI: 10.1016/j.pmrj.2016.03.008.
20. Rabago D, Mundt M, Zgierska A, Grettie J. Hypertonic dextrose injection (prolotherapy) for knee osteoarthritis: Long term outcomes. Complement Ther Med. 2015;23(3):388-95. DOI: 10.1016/j.ctim.2015.04.003.
21. Waluyo Y, Artika SR, Wahyuni IN, Adnan E, Budu, Bukhari A. Functional outcome in knee osteoarthritis after dextrose prolotherapy intervention: A severity-based pilot study. JKKI. 2023(1):47-54. DOI: 10.20885/JKKI.Vol14.Iss1.art8.
22. Sit RWS, Wu RWK, Rabago D, Reeves KD, Chan DCC, Yip BHK, et al. Efficacy of Intra-Articular Hypertonic Dextrose (Prolotherapy) for Knee Osteoarthritis: A Randomized Controlled Trial. Ann Fam Med. 2020;18(3):235-42. DOI: 10.1370/afm.2520.
23. Sert AT, Sen EI, Esmaeilzadeh S, Ozcan E. The Effects of Dextrose Prolotherapy in Symptomatic Knee Osteoarthritis: A Randomized Controlled Study. J Altern Complement Med. 2020;26(5):409-17. DOI: 10.1089/acm.2019.0335.
24. Rabago D, Patterson JJ, Mundt M, Kijowski R, Grettie J, Segal NA, et al. Dextrose Prolotherapy for Knee Osteoarthritis: A Randomized Controlled Trial. Ann Fam Med. 2013;11(3):229-37. DOI: 10.1370/afm.1504.
25. Teymouri A, Birang N, Fakheri M, Nasiri A. Comparison of the efficacy of ultrasound-guided dextrose 25% hypertonic prolotherapy and intra-articular normal saline injection on pain, functional limitation, and range of motion in patients with knee osteoarthritis; a randomized controlled trial. BMC Musculoskelet Disord. 2025;26(1):313. DOI: 10.1186/s12891-025-08580-5.
26. Yildiz K, Guler H, Ogut H, Yildizgoren M, Turhanoglu A. A comparison between hypertonic dextrose prolotherapy and conventional physiotherapy in patients with knee osteoarthritis. Med Int. 2023;3(5):45. DOI: 10.3892/mi.2023.105.
27. Meena RK, Soni P, Meena MK. Evaluating the Effectiveness of Prolotherapy Compared to Non-Surgical Alternatives in Treating Knee Osteoarthritis. Int J LifeSci Biotechnol Pharma Res. 2024;13(5):34-8.
28. Bayat M, Hojjati F, Boland Nazar NS, Modabberi M, Rahimi MS. Comparison of Dextrose Prolotherapy and Triamcinolone Intraarticular Injection on Pain and Function in Patients with Knee Osteoarthritis - A Randomized Clinical Trial. Anesth Pain Med. 2023;13(2):e134415. DOI: 10.5812/aapm-134415.
29. Arias-Vázquez PI, Tovilla-Zárate CA, Legorreta-Ramírez BG, Burad Fonz W, Magaña-Ricardez D, González-Castro TB, et al. Prolotherapy for knee osteoarthritis using hypertonic dextrose vs other interventional treatments: systematic review of clinical trials. Adv Rheumatol. 2019;59(1):39. DOI: 10.1186/s42358-019-0083-7.
30. Wee TC, Neo EJR, Tan YL. Dextrose prolotherapy in knee osteoarthritis: A systematic review and meta-analysis. J Clin Orthop Trauma. 2021;19:108-17. DOI: 10.1016/j.jcot.2021.05.015.
31. Waluyo Y, Artika SR, Insani Nanda Wahyuni, Gunawan AMAK, Zainal ATF. Efficacy of Prolotherapy for Osteoarthritis: A Systematic Review. J Rehabil Med. 2023;55:jrm00372. DOI: 10.2340/jrm.v55.2572.
32. Liao CD, Chen HC, Huang MH, Liou TH, Lin CL, Huang SW. Comparative Efficacy of Intra-Articular Injection, Physical Therapy, and Combined Treatments on Pain, Function, and Sarcopenia Indices in Knee Osteoarthritis: A Network Meta-Analysis of Randomized Controlled Trials. Int J Mol Sci. 2023;24(7):6078. DOI: 10.3390/ijms24076078.
33. Gül D, Orsçelik A, Akpancar S. Treatment of Osteoarthritis Secondary to Developmental Dysplasia of the Hip with Prolotherapy Injection versus a Supervised Progressive Exercise Control. Med Sci Monit. 2020;26:e919166. DOI: 10.12659/MSM.919166.
34. Bertrand H, Reeves KD, Bennett CJ, Bicknell S, Cheng AL. Dextrose Prolotherapy Versus Control Injections in Painful Rotator Cuff Tendinopathy. Arch Phys Med Rehabil. 2016;97(1):17-25. DOI: 10.1016/j.apmr.2015.08.412.
35. Nagori SA, Jose A, Gopalakrishnan V, Roy ID, Chattopadhyay PK, Roychoudhury A. The efficacy of dextrose prolotherapy over placebo for temporomandibular joint hypermobility: A systematic review and meta-analysis. J Oral Rehabil. 2018;45(12):998-1006. DOI: 10.1111/joor.12698.
36. Fu K, Robbins SR, McDougall JJ. Osteoarthritis: the genesis of pain. Rheumatology (Oxford). 2018;57:iv43-50. DOI: 10.1093/rheumatology/kex419.